Health communication
CONTENTS
Hemorrhoids
1. Definition
Internal hemorrhoids originate from the superior hemorrhoidal venous plexus located above the dentate line. There are usually three principal hemorrhoidal cushions situated at the 3 o’clock (left lateral), 8 o’clock (right posterior), and 11 o’clock (right anterior) positions. In addition, accessory hemorrhoidal cushions may be present between the main ones.
External hemorrhoids arise from the inferior hemorrhoidal venous plexus below the dentate line and are covered by skin. The superior hemorrhoidal venous plexus drains into the superior rectal vein and then into the portal venous system, whereas the inferior hemorrhoidal venous plexus drains into the systemic venous circulation. These two venous plexuses communicate with each other.
Mixed hemorrhoids occur when internal and external hemorrhoids are contiguous and connected.
Circumferential hemorrhoids occur when the major and accessory hemorrhoidal cushions coalesce to form a circumferential prolapse.
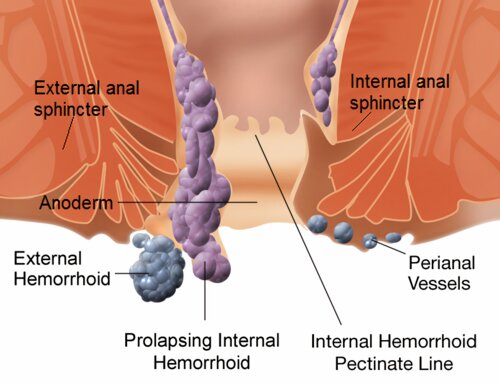
Figure 1. Internal and external hemorrhoids.
2. Epidemiology
Hemorrhoidal disease is common worldwide. Many international statistics indicate that the prevalence in individuals older than 50 years is approximately 50%, and that about 5% of the general population is affected. The incidence of hemorrhoidal disease increases with age. The prevalence in males is approximately twice that in females.
Epidemiologic studies have reported prevalence rates of 13.1% in Ethiopia (2021), 16% in Israel (2009), 14.4% in South Korea (2014), 18% in Egypt (2011), and 38.9% in Austria (2019).
Risk factors
- - Chronic colitis and chronic constipation
- - Increased intra-abdominal pressure, as seen in chronic bronchitis, bronchiectasis, and heavy manual labor such as carrying heavy loads
- - Prolonged standing posture, such as in sales personnel, office secretaries, and tailors
- - Venous obstruction caused by rectal cancer, pelvic tumors, or advanced pregnancy.
3. Pathophysiology
Venous congestion and hypertrophy of the hemorrhoidal cushions above the dentate line give rise to internal hemorrhoids. Because these cushions communicate with veins located below the dentate line, external hemorrhoids may also develop. Recurrent episodes of venous congestion cause progressive dilation of the rectal mucosa and perineal skin, resulting in downward prolapse.
Several pathophysiologic mechanisms have been proposed for hemorrhoidal disease:
- Dysregulation of the arteriovenous shunts within the anal cushions
- Impaired venous return through the superior hemorrhoidal veins, resulting in progressive enlargement of the hemorrhoidal cushions
- Increased intra-abdominal pressure during straining, difficult urination, or pregnancy, which impedes venous return and enlarges the cushions
- Prolonged hypertonicity of the anal sphincter, which reduces venous drainage through trans-sphincteric shunts and contributes to dilatation of the hemorrhoidal cushions.
4. Clinical Manifestations
Bleeding
Bleeding is the most common symptom. Initially, it may be slight and only detected as blood on toilet paper or a few streaks of blood coating hard stool. In more severe cases, bleeding may occur as dripping blood or even as spurting hemorrhage.
Prolapse
Prolapse is also a common symptom. According to the degree of prolapse, internal hemorrhoids are classified into four grades. Grade III and grade IV prolapse cause significant anal discomfort, and the anus is often persistently moist.
Pain
Pain is less common. It may result from:
- Thrombosis: small blood clots develop within the hemorrhoidal cushion; patients often sit leaning to one side
- Strangulated prolapsed hemorrhoids: causing marked edema and swelling
- Associated anal fissure: due to excessive straining; once an anal fissure occurs, the pain is usually severe
- Associated abscess: located either immediately beneath the mucosa or within the ischioanal fossa.
Physical findings
For internal hemorrhoids, grade I and grade II lesions are usually not visible on inspection. In grade III disease, if the anal margins are widely separated or the patient is asked to strain forcefully, purplish, bulging hemorrhoidal cushions may be seen, typically at the 4, 8, and 11 o’clock positions. In grade IV disease, the hemorrhoids remain prolapsed permanently; when extensive and bilateral, they may resemble a rosette.
For external hemorrhoids, visible protrusions are present at the anal verge, causing loss of the normal skin folds. Depending on the stage of disease, complications such as thrombosis, infection, or fibrosis with residual skin tags may be observed.
5. Complications
Infection: papillitis and cryptitis
These complications are clinically manifested by a burning sensation and pruritus in the anal region. Digital rectal examination is very painful and reveals poor sphincter relaxation. Anoscopy shows edematous, whitish anal papillae, and the crypts between the hemorrhoidal cushions may appear as shallow red ulcerations.
Thrombosis
Thrombosis occurs when blood clots form within the hemorrhoidal cushions. It presents as a painful swollen perianal mass, with pain being most severe within the first 48 hours and usually decreasing significantly after day 4 or 5. With natural evolution, pressure from the underlying clot may cause necrosis of the overlying skin, after which the clot may extrude spontaneously, or it may gradually resolve, with recovery occurring after 10–14 days. A residual skin tag may form several weeks later.
- Internal thrombosed hemorrhoids: severe pain with a sensation of a foreign body in the anal canal. Digital rectal examination reveals a small, round, firm, and very tender nodule. Anoscopy shows purplish protrusions.
- External thrombosed hemorrhoids: usually more painful than thrombosed internal hemorrhoids. A pale bluish swollen mass is visible, obliterating the normal perianal skin folds. It is extremely tender on palpation. If incised, a small clot may be expressed, with immediate pain relief.
Prolapse and strangulation
Internal hemorrhoids may prolapse beyond the anal canal and become incarcerated, making manual reduction impossible. The prolapsed hemorrhoidal mass may be partially or completely strangulated.
Fibrosis
Fibrosed hemorrhoidal cushions evolve into skin tags. These tags are painless and do not bleed, but they may cause discomfort or difficulty with hygiene.
6. Treatment
6.1. Principles of treatment
- Only symptomatic hemorrhoidal disease requires treatment
- Treatment is indicated when symptoms interfere with daily activities or work
- Surgery is reserved for cases in which medical treatment and office-based procedures fail, or when complications occur.
6.2. Modern treatment of hemorrhoidal disease
6.2.1. Medical treatment
All grade I and grade II internal hemorrhoids can be managed conservatively with topical medication and dietary modification.
- A high-fiber diet rich in vegetables and fruits, together with adequate fluid intake
- Oral or rectal laxatives to facilitate defecation, such as Fructines, Forlax, Microlax, and Normacol
- Suppositories or creams administered into the anal canal, which mainly relieve pain and produce an astringent effect on the mucosa
- Venoactive agents and hemorrhoidal medications such as Daflon, Mastu-S, Mastu-S Forte, Proctolog, Procto-Glyvenol, and Preparation H
- In prolapsed and markedly edematous internal hemorrhoids, gentle manual reduction into the anal canal may be attempted, followed by topical astringents, bed rest, and warm sitz baths.
6.2.2. Injection sclerotherapy
Principle: a sclerosing chemical solution, such as 5% phenol in vegetable oil or polidocanol, is injected into the loose submucosal tissue above the hemorrhoidal cushion. This induces inflammation and fibrosis, causing fixation to the underlying muscle layer and reducing blood supply to the hemorrhoid, thereby shrinking it.
Technique: under anoscopic guidance, 2 mL of sclerosant is injected into the submucosa above the dentate line at the base of the internal hemorrhoid.
Complications: ulceration, abscess, prostatitis, and drug allergy.
Indications: grade I and grade II internal hemorrhoids.
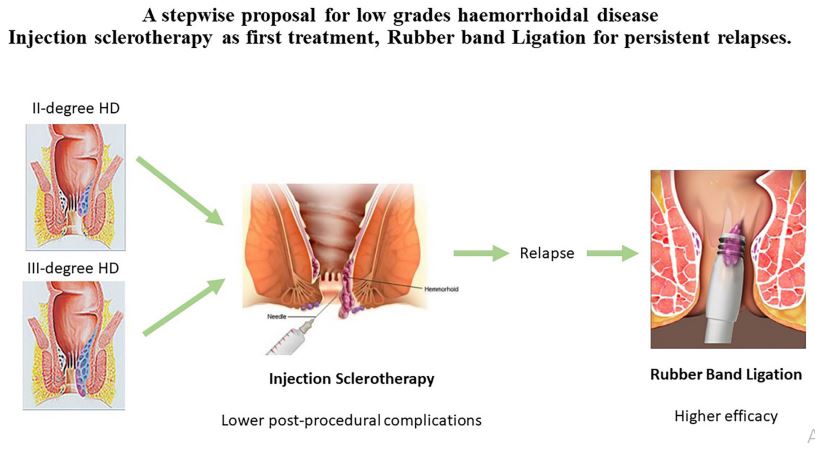
Figure 2. Hemorrhoid treatment methods: sclerotherapy and rubber band ligation.
6.2.3. Rubber band ligation
Principle: an elastic band is placed around the base of the hemorrhoid in the mucosal region, producing ischemia, necrosis, and fibrosis over several days.
Technique: under anoscopic visualization, the hemorrhoid is grasped and an elastic band is applied at its base using a ligator. Usually, one hemorrhoidal cushion is treated at a time, with subsequent sessions performed after 2–4 weeks if needed.
Complications: pain if the procedure is improperly performed, particularly if the band is placed below the dentate line. Infection and bleeding may also occur, with bleeding typically occurring between days 7 and 10.
Indications: grade II and grade III internal hemorrhoids.
6.2.4. Cryotherapy
Principle: freezing induces necrosis of the hemorrhoidal tissue.
Technique: under anoscopy, a cryoprobe is applied to the hemorrhoid and cooling is achieved with CO₂ or N₂O at temperatures of approximately 600–1500°C below zero for 10–15 minutes. All hemorrhoidal cushions may be treated in a single session.
Complications: the main inconvenience is anal discharge for several hours after the procedure, which may persist for 4–6 weeks. Bleeding occurs in approximately 3% of cases. Moreover, satisfactory outcomes are reported in only 45%–88% of patients.
Indications: grade I and grade II internal hemorrhoids.
6.2.5. Surgery
Principle: excision and ligation of the hemorrhoidal cushions close to their base, while avoiding anal stenosis and preserving sphincter integrity.
Milligan–Morgan hemorrhoidectomy: excision of the principal hemorrhoidal cushions while preserving mucocutaneous bridges between them.
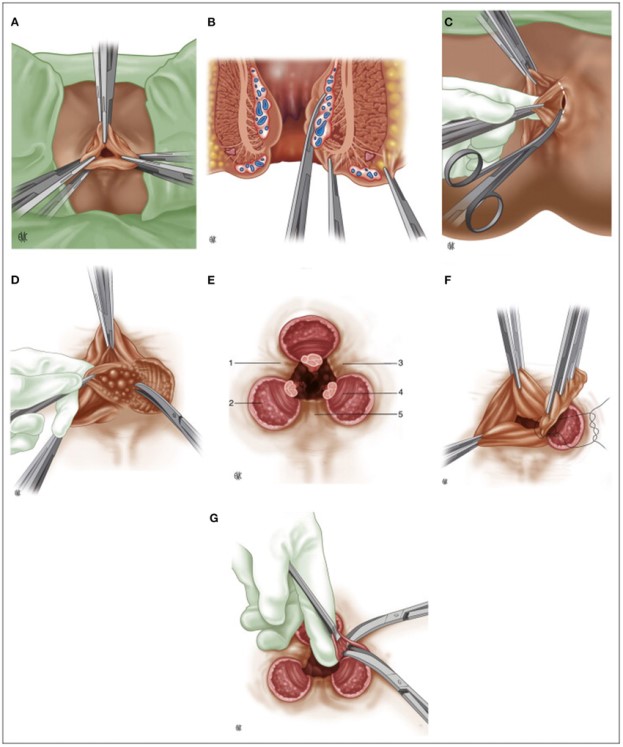
Figure 3. Surgical treatment of hemorrhoids: Milligan–Morgan technique.
Ferguson hemorrhoidectomy (closed hemorrhoidectomy): excision of each hemorrhoidal cushion followed by closure of the mucocutaneous defect.
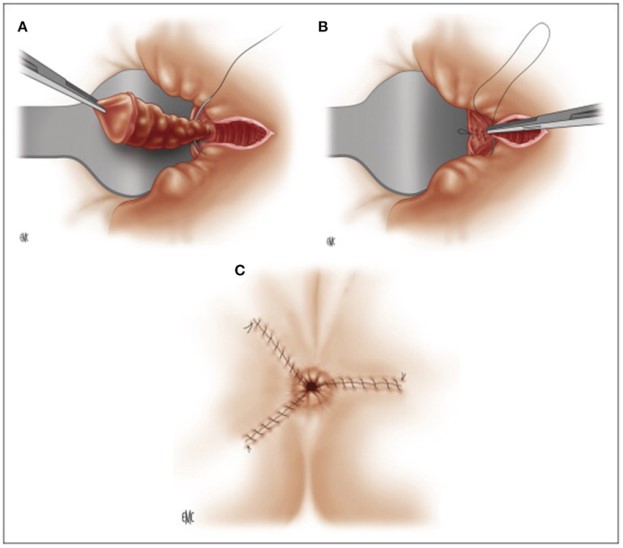
Figure 4. Surgical treatment of hemorrhoids: Ferguson technique.
Whitehead procedure: circumferential excision of the mucosa and submucosa containing the hemorrhoidal venous plexus, followed by advancement of the proximal mucosa and suturing to the perianal skin. Because of numerous complications, including severe pain, fecal incontinence, anal discharge, and anal stenosis, this technique is now rarely used.
Longo stapled hemorrhoidopexy:
- Principle: circumferential resection of a ring of rectal mucosa reduces blood flow to the hemorrhoidal plexus, thereby decreasing hemorrhoidal volume, while simultaneously lifting the anal cushions back into the anal canal using a 33-mm circular stapler.
- Indications: grade II and grade III internal hemorrhoids.
Doppler-guided hemorrhoidal artery ligation:
This technique was first performed by Kazumasa Morinaga in 1995. A Doppler ultrasound probe is used to identify six terminal branches of the superior rectal artery, which are then ligated approximately 2 cm above the dentate line. This reduces blood flow to the hemorrhoidal cushions, decreases their volume, and preserves the anal cushions.
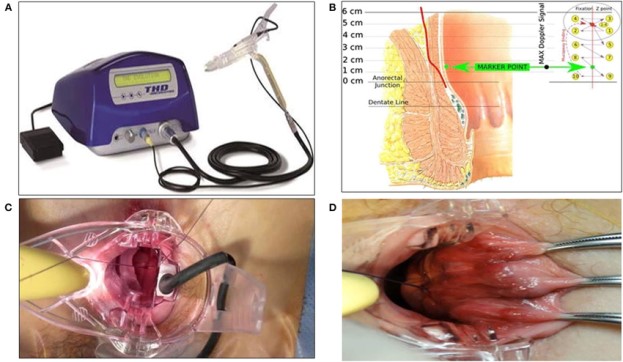
Figure 5. Surgical treatment of hemorrhoids: Doppler-guided hemorrhoidal artery ligation.
Postoperative complications
- Urinary retention: the most common complication
- Bleeding: early postoperative bleeding within the first 48 hours occurs in approximately 1%–2% of cases; delayed bleeding at 7–10 days may result from infection or sloughing of the hemorrhoidal pedicle
- Postoperative pain, due to surgery in a highly sensitive region and possible suturing involving the sphincter
- Edema or delayed wound healing
- Fecal incontinence due to sphincter injury.
Postoperative care
- Analgesia: NSAIDs and paracetamol
- Antibiotics: ampicillin 1 g twice daily plus gentamicin 0.08 g/day for 5–7 days; metronidazole 500 mg three times daily for 5–7 days
- Laxatives
- Sitz bath twice daily
- Daily digital examination of the anal canal to prevent anal stenosis.
7. Prevention
- Early detection of hemorrhoidal disease, especially in patients with rectal bleeding
- Examination and treatment of conditions that increase intra-abdominal pressure, such as bronchitis, chronic cough, or colitis
- Prevention of constipation by adequate fluid intake and a diet rich in green vegetables and fresh fruits, especially papaya, oranges, mandarins, and grapefruit
- Regular physical activity and correction of factors associated with hemorrhoidal disease
- Limitation of irritating spicy foods and constipation-promoting substances, especially chili, alcohol, and coffee
- Avoidance of prolonged sitting and heavy lifting
- Careful postoperative follow-up and wound care to prevent complications such as anal stenosis and to detect complications promptly if they occur.
REFERENCES
- Russell TR. Anorectum, hemorrhoids. In: Current Surgical Diagnosis and Treatment. 10th ed. 1994;693–697.
- Wexner SD, Fleshman JW. Colon and Rectal Surgery—Anorectal Operations. 2012.
- Tutino R, et al. A stepwise proposal for low-grade hemorrhoidal disease: injection sclerotherapy as a first-line treatment and rubber band ligation for persistent relapses. Front Surg. 2022;8:782800.
- Rubbini M, Ascanelli S. Classification and guidelines of hemorrhoidal disease: present and future. World J Gastrointest Surg. 2019;11(3):117.
- Pata F, et al. Evolution of surgical management of hemorrhoidal disease: an historical overview. Front Surg. 2021;8:727059.
MSc. Kim Ngoc Son
MSc. Ong Thi tuyet