Health communication
CONTENTS
Rabies
1. Causative Agent
Rabies virus belongs to the family Rhabdoviridae, genus Lyssavirus. It is an RNA virus with a lipid envelope. Rabies virus has low environmental resistance and is readily inactivated by heat. It is easily destroyed by lipid solvents such as soap, ether, chloroform, and acetone, and is highly sensitive to ultraviolet light. It is also rapidly inactivated in alcohol and iodinated alcohol solutions.
The virus measures approximately 80 × 180 nm and consists of a single RNA strand. It has a cylindrical shape with one conical end and one flat end, giving it the characteristic appearance of a bullet.
The virus contains five proteins (Figure 1):
- Glycoprotein (G protein): molecular weight approximately 67,000; located in the viral envelope, which bears spikes measuring 6–8 nm in length. Glycoprotein induces the production of neutralizing antibodies.
- Nucleocapsid (N protein): molecular weight approximately 56,000; forms the viral core and induces complement-fixing antibodies but not neutralizing antibodies.
- Viral polymerase (L protein)
- Phosphoprotein (P protein): molecular weight approximately 38,000; a membrane-associated protein closely linked to the nucleocapsid.
- Matrix protein (M protein): molecular weight approximately 26,000; associated with the surrounding lipoprotein structure of the virion.
-
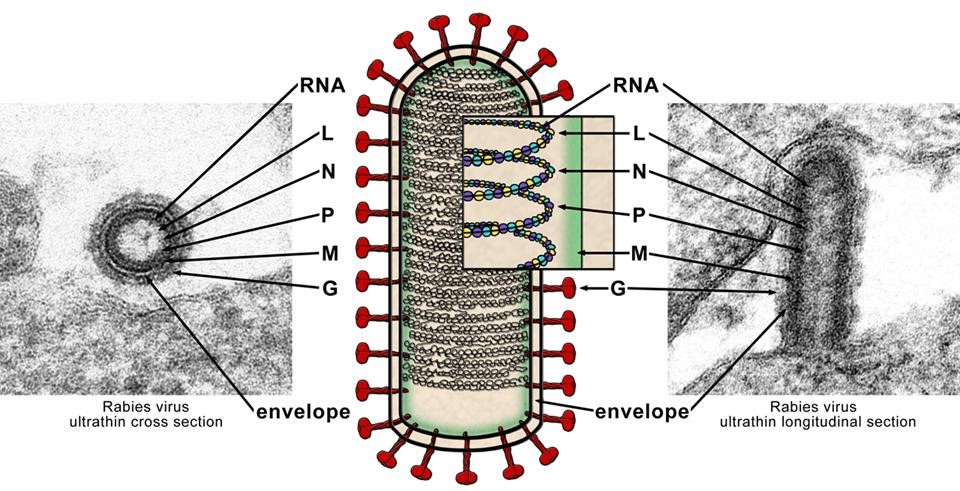
Figure 1. Structure of rabies virus
2. Epidemiology
Approximately 59,000 people die of rabies each year worldwide, of whom 95% are in Asia and Africa. Around 99% of human rabies cases are transmitted by dogs. Rabies has now been eliminated in Western Europe, Canada, the United States, Japan, Australia, and several Latin American countries.
In Asia, approximately 35,172 people die from rabies annually, with India accounting for 59.9% of these deaths. Reports indicate approximately 1,875 deaths each year in Central Asia and 229 in the Middle East due to rabies. In Africa, an estimated 21,476 people die annually from dog-mediated rabies.
The total economic burden of dog-mediated rabies is estimated at USD 8.6 billion.
3. Pathogenesis
After entering the body through a bite wound, rabies virus remains near the site of inoculation for a period of time and then replicates in muscle cells. Unless inactivated by natural host defenses or active immune mechanisms, the virus enters the axons of peripheral neurons. From there, it travels centripetally to the spinal ganglia and brain. Once it reaches the central nervous system, the virus spreads centrifugally and becomes present in neurons throughout the body. It may then be detected by fluorescent antibody testing in corneal cells or skin biopsy specimens.
The virus is present in saliva, urine, and cerebrospinal fluid. The highest viral concentrations are found in the brain, particularly in the brainstem, basal ganglia, hippocampus, and cerebellum. The virus may also be found in tissues such as skeletal muscle, myocardium, adrenal medulla, kidneys, pancreas, and nerve fibers associated with hair follicles.
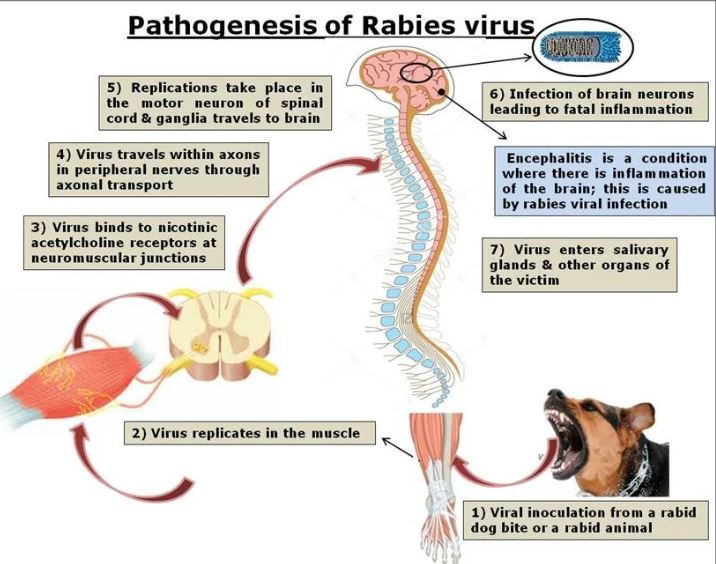
Figure 2. Pathogenesis of rabies virus
4. Clinical Manifestations
4.1. Rabies in animals
Rabies virus may be present in the saliva of rabid animals before clinical signs appear. The duration of this preclinical shedding period varies depending on the animal species and viral strain. For example, in dogs it ranges from approximately 4 to 12 days, in cats about 1 day, and in bats about 10 days.
Rabies in dogs
The incubation period in dogs is usually 3 to 12 weeks, but may range from 5 days to 14 months. The disease occurs in two forms: furious rabies and paralytic rabies (Figure 4).
- Furious form: accounts for about 25% of cases. The earliest sign is a change in behavior, followed by difficulty swallowing, protrusion of the tongue, altered bark, and either depression with isolation or snapping at imaginary objects. Subsequently, the dog becomes highly restless, leaves home, bites even inanimate objects, barks in a howling manner, drools excessively, and eventually dies.
- Paralytic form: characterized by paralysis of the lower jaw, causing a dropped jaw and drooling, followed by paralysis of the hind limbs, then forelimbs, then bulbar paralysis, inability to bark, and death.
Dogs usually die within 3 to 7 days after disease onset. Cats are less commonly affected than dogs. Rabies in cats has a similar course to that in dogs; affected cats often hide in secluded places or become unusually vocal, restless, and aggressive when touched.
4.2. Rabies in humans
Incubation period
The incubation period is typically 20 to 60 days but may range from 4 days to several years. It is shorter when the bite is located on the face or when transmission occurs through corneal transplantation.
Prodromal stage
- Fatigue, anorexia, headache, malaise, fever, myalgia
- Itching, pain, or paresthesia at the bite site, which is often already healed
- Personality or mood changes: patients may feel apprehensive, anxious, irritable, sleepless, agitated, or depressed
- Less common symptoms include cough, chills, sore throat, abdominal pain, nausea, vomiting, diarrhea, and dysuria.
Acute neurologic stage
Rabies presents in two major clinical forms: furious rabies and paralytic rabies.
Furious rabies
- Most patients develop hydrophobia due to painful spasms of the respiratory muscles.
- Spasms of the larynx and respiratory muscles are usually abrupt and severe; the neck and back arch, and the arms may flail upward. Patients may also develop aerophobia, photophobia, and hypersensitivity to visual or olfactory stimuli.
- Because of marked hyperexcitability, patients often have episodes of delirium, disorientation, bizarre behavior, fleeing, or aggression toward others. During attacks lasting several minutes, they may thrash, bite, howl like a dog, breathe rapidly and irregularly, and may die during the episode.
- Patients may have high fever up to 40°C, dilated pupils, anisocoria, hypersalivation, lacrimation, profuse sweating, and orthostatic hypotension. Excessive salivation combined with dysphagia results in spitting and frothing at the mouth.
- Between episodes, patients may remain alert and relatively cooperative. However, the disease progresses rapidly to coma or sudden cardiac or respiratory arrest. Death usually occurs within 2 to 4 days after the onset of furious rabies.
Paralytic rabies
This form accounts for approximately 20% of cases and is often seen in patients who have received rabies vaccination after an animal bite. Initial manifestations may include paresthesia at the bite site, spinal pain, and pain radiating from the bitten limb. Paralysis then progresses upward to the upper limbs, with loss of deep tendon reflexes. Patients develop urinary retention and constipation, followed by paralysis of the neck, face, and tongue muscles leading to aspiration, then paralysis of the respiratory muscles. Death occurs more slowly than in furious rabies and may be delayed for 2 to 20 days.
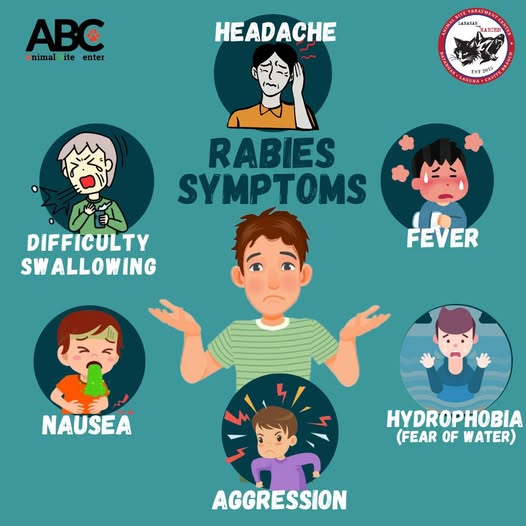
Figure 3. Clinical manifestations of rabies in humans
5. Laboratory findings
- Antigen detection by fluorescent antibody test (FAT)
- Virus isolation
- Molecular techniques such as RT-PCR
- Antibody detection by ELISA, RFFIT, and FAVN.
6. Complications
Respiratory system
- Asphyxia, hypoxia, and respiratory arrest
- Pneumonia, bronchopneumonia
- Pneumothorax.
Cardiovascular system
- Supraventricular tachycardia, sinus bradycardia, atrioventricular block, sick sinus syndrome
- Hypotension, acute pulmonary edema, heart failure, and shock due to myocarditis.
Nervous system
- Increased intracranial pressure due to cerebral edema or hydrocephalus.
Gastrointestinal system
- Stress-related gastrointestinal ulceration with hematochezia or gastrointestinal bleeding.
7. Diagnosis
Diagnosis is based on:
- A history of exposure to a rabid or suspected rabid animal
- Compatible clinical manifestations
- Specific laboratory testing.
8. Prevention
8.1. Vigilance regarding animals at risk of transmitting rabies
Never attempt to touch, pet, or hold unfamiliar domestic animals or wild animals.
8.2. Control of suspected rabid animals
- Take precautions against rabid dogs.
- Destroy domestic animals or livestock bitten by rabid animals.
- For animals suspected of having rabies that have bitten humans:
- Confine and observe the animal for 10 days.
- If the animal has been killed, beaten to death, or already shows signs of rabies, it should be submitted for laboratory confirmation.
8.3. Pre-exposure prophylaxis
Pre-exposure vaccination is recommended for:
- Veterinarians
- Laboratory personnel working with rabies virus
- Dog slaughter workers
- People living in endemic areas
- Travelers to rabies-endemic regions.
Booster vaccination should be given periodically to individuals with ongoing risk of rabies exposure.
8.4. Wound management
8.5. Post-exposure prophylaxis
According to World Health Organization (WHO) recommendations, post-exposure prophylaxis includes:
- Immediate wound care
- Rabies vaccination
- Rabies immunoglobulin administration for category III exposure.
WHO exposure categories
- Category I: touching or feeding animals, licks on intact skin
- Category II: minor scratches or abrasions without bleeding, licks on broken skin
- Category III: single or multiple transdermal bites or scratches, contamination of mucous membranes or wounds with saliva, or wounds near the central nervous system or in areas rich in nerve supply.
Rabies immunoglobulin
Principle: rabies immunoglobulin should be administered as soon as possible after exposure and should be given only once during treatment.
It should be infiltrated as much as anatomically feasible into and around the wound so that the immunoglobulin penetrates deeply into the affected area. Any remaining volume should be administered by deep intramuscular injection at a site distant from the rabies vaccine injection site.
Recommended doses:
- Human rabies immunoglobulin (HRIG): 20 IU/kg body weight
- Equine rabies immunoglobulin (ERIG): 40 IU/kg body weight.
REFERENCES
- Bleck TP, Rupprecht CE. Principles and Practice of Infectious Diseases, 6th edition, 2005. In: Mandell, Douglas, and Bennett. Churchill Livingstone. Chapter 160, pp. 2047–2054.
- Hanlon CA, Corey L. Rabies virus and other rhabdoviruses. Harrison’s Principles of Internal Medicine, 16th edition, 2005, pp. 1155–1160.
- Binder LS. Rabies. Emergency Medicine, 1992. Chapter 84, pp. 527–529.
- Abraham S, Ravindran J, Abishaw N, Sandam NP, Thimmareddy P, Govindaraju G. Review on rabies and vaccines. Int J Curr Microbiol App Sci. 2017;6(12):2064–2085.
- World Health Organization. Rabies vaccines and immunoglobulins: WHO position paper, April 2018.
- Virus structure. WHO Rabies Bulletin.
- Epidemiology and burden. World Health Organization.
- Rabies in dogs. PDSA.
- Signs and symptoms of rabies. Rabies Alliance.
- Can rabies be eliminated? Rabies Alliance.
MSc. Kim Ngoc Son
MSc. Tran Khanh