Health communication
CONTENTS
Diphtheria
1. General Overview
Diphtheria is an infectious and toxigenic disease, transmitted via the respiratory route and capable of causing outbreaks, caused by Corynebacterium diphtheriae. It commonly affects children under 15 years of age and individuals lacking immunity because they have not been fully vaccinated. The organism typically colonizes and damages the upper respiratory tract (nose, pharynx, and larynx), producing an adherent pseudomembrane that is difficult to remove, and releases exotoxin causing systemic toxicity involving the heart, kidneys, and nervous system. The disease carries a high risk of death due to airway obstruction and myocarditis. Specific treatment includes antibiotics and diphtheria antitoxin (DAT), and prevention is possible through vaccination.
2. Causative Agent
Corynebacterium diphtheriae is a Gram-positive bacillus, club-shaped, measuring approximately 1–9 µm in length and 0.3–0.8 µm in width. It is non-motile, non-encapsulated, and non-spore-forming. The organism can survive for prolonged periods in pseudomembranes and in the pharynx of infected patients. In low-light conditions, it may survive for up to 6 months and can persist for long periods on contaminated objects such as children’s toys and healthcare workers’ gowns. The bacterium is killed at 58°C within 10 minutes and dies within a few hours under direct sunlight.
Figure 1. Corynebacterium diphtheriae
3. Epidemiology
3.1. Source of infection
Humans are the only known reservoir of infection.
3.2. Mode of transmission
Diphtheria is transmitted from person to person, including transmission from both symptomatic patients and asymptomatic carriers. The main route of transmission is through respiratory droplets or direct contact with respiratory secretions or secretions from infected skin lesions. Some infected individuals become carriers and may continue to harbor C. diphtheriae for weeks or months, or more rarely, for many years or even for life. The incubation period is usually 2–5 days; however, disease onset may occur as late as 10 days after exposure.
3.3. Disease distribution
Diphtheria occurs in many parts of the world, especially in tropical countries. Today, it is a rare disease in developed countries with high vaccine coverage. During the period 2011–2021, the World Health Organization (WHO) recorded a total of 101,699 diphtheria cases worldwide, of which more than 60,000 occurred in Southeast Asia. In Vietnam, the number of diphtheria cases increased from 13 in 2018 to 237 in 2020. In the South Central Coast region alone, 28 cases were reported, most of them in children aged 5 years and older. By 2023, Vietnam had reported 57 cases nationwide, including 7 deaths, mainly in the final months of the year and concentrated in the provinces of Ha Giang, Dien Bien, and Thai Nguyen.
4. Pathogenesis
Diphtheria may be fatal, primarily because of the action of diphtheria exotoxin, a polypeptide with a molecular weight of approximately 62 kDa. This exotoxin is produced only by toxigenic strains of Corynebacterium diphtheriae and is considered the principal virulence factor determining the clinical manifestations of the disease.
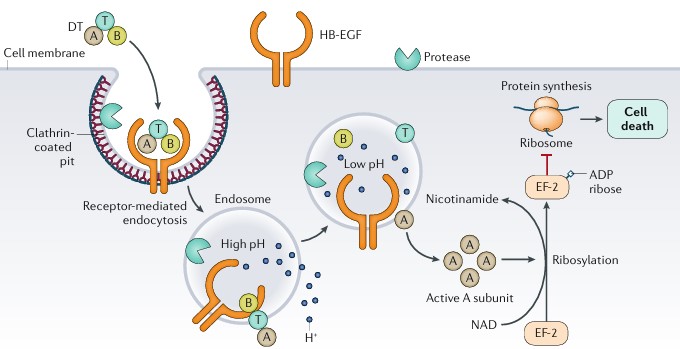
Figure 2. Mechanism of action of diphtheria toxin
The toxin is produced at the site of pseudomembrane formation on the mucosa, then enters the circulation and disseminates to multiple organs. Although it can affect nearly all cell types, diphtheria toxin causes the most severe injury to the myocardium (myocarditis), peripheral nerves (demyelination), and kidneys (acute tubular necrosis).
A characteristic feature of diphtheria is the presence of mucosal ulcerations covered by a pseudomembrane. This pseudomembrane is composed of fibrin, necrotic cells, and neutrophils. Initially, it is white and firmly adherent to the mucosa, but may gradually become gray, green, or black as necrosis progresses. These mucosal lesions result from epithelial cell necrosis induced by the toxin, accompanied by congestion, edema, and vascular obstruction in the submucosal layer. Fibrin-rich exudate from the ulcerated lesions continues to develop into a pseudomembrane, which may spread from the pharynx down to the medium-sized bronchi. In severe cases, extension and detachment of the pseudomembrane may obstruct the airway and cause death.
5. Clinical Manifestations
The most common clinical form is pharyngeal diphtheria (70%), followed by laryngeal diphtheria (20–30%), nasal diphtheria (4%), ocular diphtheria (3–8%), and cutaneous diphtheria.

Figure 3. Clinical manifestations of diphtheria
5.1. Pharyngeal diphtheria
Incubation period
The incubation period is 2–5 days, during which there are no clinical symptoms.
Prodromal stage
- Patients usually develop a temperature of 37.5–38°C, sore throat, malaise, fatigue, poor appetite, mild pallor, and unilateral or bilateral rhinorrhea, which may be blood-stained.
- On examination of the throat, there is mild erythema, and one tonsil may show a faint white spot suggestive of early pseudomembrane formation. Small, mobile, non-tender cervical lymph nodes may be palpable.
Fully developed stage
This stage usually begins on the second or third day of illness.
- Systemic findings: patients have a temperature of 38–38.5°C, odynophagia, pallor, marked fatigue, anorexia, tachycardia, and mildly reduced blood pressure.
- Throat findings: the pseudomembrane extends over one or both tonsils; in severe cases, it may spread to cover the uvula and soft palate. Initially pearly white, it later becomes pale yellow, remains firmly adherent to the mucosa, and bleeds when removal is attempted; if removed, it reforms rapidly within a few hours. The membrane is tough, does not dissolve in water, and the surrounding mucosa appears normal.
- The angle-of-jaw lymph nodes are enlarged and tender. Patients often have profuse rhinorrhea, with white or purulent nasal discharge.
5.2. Malignant diphtheria
This form may appear as early as days 3–7 of illness. It is characterized by severe infection and toxemia, high fever of 39–40°C, and extensive pseudomembrane formation involving the pharynx and lips. Marked cervical lymphadenopathy and soft tissue edema produce the so-called “bull neck” appearance. Early complications commonly include myocarditis, renal failure, and neurologic injury.
5.3. Laryngeal diphtheria
- Isolated laryngeal diphtheria is uncommon; it usually occurs as pharyngo-laryngeal diphtheria.
- Clinical manifestations include acute laryngitis, characterized by a barking cough, hoarseness, inspiratory dyspnea with stridor, and in advanced stages, asphyxia.
6. Laboratory findings
6.1. Etiologic diagnosis
- Specimen collection: a throat swab is obtained from the margin surrounding the pseudomembrane. The swab should be placed in Amies or Stuart transport medium and sent to the laboratory as soon as possible.
- Microscopy: Gram stain may demonstrate club-shaped Gram-positive bacilli.
- Culture: specimens are cultured on blood agar and on selective media such as Loeffler medium and potassium tellurite medium, or cystine tellurite blood agar (CTBA), to isolate C. diphtheriae. Toxigenicity testing may then be performed, for example by the Elek test.
- PCR: polymerase chain reaction may be used, where available, to detect the diphtheria toxin gene.
6.2. Routine investigations
Routine tests may include complete blood count, liver enzymes, cardiac enzymes, urea, creatinine, electrolytes, blood glucose, arterial blood gas when indicated, electrocardiography, urinalysis, and chest radiography.
7. Diagnosis
7.1. Suspected case
- Clinical criteria: clinical features consistent with diphtheria, with pseudomembrane formation in the pharyngeal region.
- Epidemiologic criteria: the patient has traveled to or come from an area with an ongoing diphtheria outbreak or an area that has had a diphtheria outbreak within the past 5 years.
7.2. Confirmed diagnosis
A suspected case with a positive laboratory test for Corynebacterium diphtheriae is considered confirmed.
7.3. Differential diagnosis
Tonsillitis with exudative pseudomembrane due to other causes
- Group A streptococcal infection
- Vincent angina
- Epstein–Barr virus (EBV) infection
- Oropharyngeal candidiasis
Laryngitis due to other causes
- Viral laryngitis
- Retropharyngeal abscess
- Anaphylaxis
Complications resembling those caused by other etiologies
- Myocarditis
- Nephritis
- Neurologic paralysis
8. Treatment
8.1. Principles of treatment
- Early detection and isolation as soon as a case is identified
- Immediate administration of diphtheria antitoxin (DAT) and antibiotics such as penicillin G, erythromycin, or azithromycin to prevent complications and reduce mortality
- Close monitoring for early detection and timely management of complications
- Comprehensive supportive care
8.2. Specific treatment
Diphtheria antitoxin (DAT)
DAT should be administered immediately when diphtheria is suspected. The dose depends on disease severity rather than age or body weight. Skin testing should be performed before administration; if positive, desensitization using the Besredka method is recommended.
- Pharyngeal or laryngeal diphtheria within the first 2 days: 20,000–40,000 IU
- Nasopharyngeal diphtheria: 40,000–60,000 IU
- Malignant diphtheria: 80,000–100,000 IU
In severe cases, intravenous DAT may be considered, with close monitoring for anaphylaxis and readiness for emergency treatment if needed. For infusion, the entire dose of DAT is diluted in 250–500 mL of 0.9% saline and administered slowly over 2–4 hours.
Antibiotics
- Penicillin G: 50,000–100,000 units/kg/day intramuscularly in 2 divided doses for 14 days or until the pseudomembrane disappears.
- Or erythromycin orally: children 30–50 mg/kg/day; adults 500 mg four times daily for 14 days or until the pseudomembrane disappears.
- Or azithromycin: children 10–12 mg/kg/day; adults 500 mg/day for 14 days.
Other supportive measures
- Respiratory support
- Hemodynamic support
- Fluid and electrolyte balance
- In patients with multiple organ failure or renal failure, continuous renal replacement therapy (CVVH) may be indicated.
- Corticosteroids may be considered in malignant diphtheria and in laryngeal diphtheria with significant edema.
- Nutritional support should be ensured.
Discharge criteria and follow-up
- The patient is clinically stable after 2–3 weeks of treatment.
- Two follow-up cultures are negative and no complications are present.
- Diphtheria vaccination must be administered after discharge.
- Outpatient follow-up should continue for 60–70 days.
9. Prevention
- All patients suspected of having diphtheria should be hospitalized and isolated until two bacteriological test results are negative. Specimens should be collected 24 hours apart and not earlier than 24 hours after initiation of antibiotic therapy. If bacteriological testing is unavailable, patients should remain isolated for 14 days after antibiotic treatment.
- Hand hygiene should be performed properly using soap or antiseptic solution.
- The patient’s home, room equipment, personal belongings, and clothing should be disinfected and decontaminated.
- Vaccination against diphtheria: children under 1 year of age should receive the 3-dose primary series at 2, 3, and 4 months of age, with booster doses at 18–24 months, 4–7 years, and 9–15 years. Older children and adults who have not been vaccinated should receive the full 3-dose primary series and subsequent boosters according to national recommendations.
- For close contacts: bacteriologic testing and follow-up for 7 days are recommended.
- A single dose of benzathine penicillin may be given (children ≤5 years: 600,000 units; children >5 years: 1,200,000 units).
- Or oral erythromycin may be used (children: 40 mg/kg/day, 10 mg per dose every 6 hours) for 7 days; adults: 1 g/day, 250 mg every 6 hours.
- Or azithromycin may be used: children 10–12 mg/kg once daily, up to a maximum of 500 mg/day; adults 500 mg/day for 7 days.
REFERENCES
- Le, H.T., Do, T.H., Dao, T.A., et al. Seroprevalence of anti-diphtheria toxoid antibody and implications for vaccination policy in Vietnam’s South-central coast: a cross-sectional study. BMC Infectious Diseases 24, 813 (2024).
- Hadfield, T. L., McEvoy, P., Polotsky, Y., Tzinserling, V. A., & Yakovlev, A. A. (2000). The pathology of diphtheria. Journal of Infectious Diseases, 181(Supplement_1), S116-S120.
- Truelove, S. A., Keegan, L. T., Moss, W. J., Chaisson, L. H., Macher, E., Azman, A. S., & Lessler, J. (2020). Clinical and epidemiological aspects of diphtheria: a systematic review and pooled analysis. Clinical Infectious Diseases, 71(1), 89-97.
MSc. Kim Ngoc Son
MSc. Tran Khanh