Health communication
CONTENTS
Appendicitis
1. History of Research
Illustrations of the appendix were first publicly published in the anatomical drawings of Berengario Da Capri and Andreas Vesalius in the sixteenth century. Earlier, Leonardo da Vinci had also depicted the appendix in his anatomical works in 1492, although these drawings were not discovered until the eighteenth century. The first documented report of appendiceal disease was made by Jean Fernel in 1544, when he performed a forensic examination on a 7-year-old child who died from perforated appendicitis caused by a quince seed. The first successful appendectomy was performed in 1736 by Claudius Amyand on an 11-year-old boy with an appendix incarcerated within an inguinal hernia.
For more than a century thereafter, typhoid and paratyphoid fever were still considered the leading causes of right iliac fossa pain. The person credited with establishing appendicitis as the leading cause of right lower quadrant pain and with introducing the term appendicitis was Reginald Heber Fitz of Harvard University in 1886. In 1889, Charles McBurney published a paper in the New York State Medical Journal describing appendicitis and advocating early laparotomy for removal of the inflamed appendix; he later introduced the McBurney incision in 1894.
In the following decades, early appendectomy became widely accepted as the gold standard treatment with broad indications to prevent perforation. By the 1970s, however, complications associated with routine appendectomy had been recognized, leading to more careful consideration of surgical indications. In 1982, Kurt Semm successfully performed the first laparoscopic appendectomy.
2. Anatomy and Physiology
The appendix develops during the eighth week of gestation. In children, the appendiceal lumen is relatively wide and conical in shape, making obstruction less likely. The appendix gradually develops and reaches a length of approximately 6–9 cm in adults. Its diameter ranges from 3–8 mm. In the elderly, the appendix gradually undergoes degeneration. The base of the appendix is the point where the three taeniae coli of the cecum converge, which serves as an important landmark for locating the appendix during surgery. The appendix is freely mobile in about 60% of cases, lies within the pelvis in about 30%, and is retrocecal in 7–10% of cases. The mucosa of the appendix is similar to that of the colon, but the appendix contains more lymphoid tissue in the submucosa. The appendix is considered an immune organ that produces immunoglobulins, particularly IgA.
3. Epidemiology
Appendicitis is currently one of the most common causes of acute surgical abdomen, with an annual incidence of approximately 100–223 cases per 100,000 population. The lifetime risk of appendicitis is about 8.6% in males and 6.7% in females worldwide. This risk is highest in individuals aged 20–40 years.
In 2019, approximately 17.7 million people worldwide had appendicitis, corresponding to a rate of 229.9 per 100,000 population. In the United States, acute appendicitis is the leading cause of acute abdominal pain requiring surgery. More than 300,000 patients in the United States are diagnosed with acute appendicitis and undergo appendectomy each year. Perforated and complicated appendicitis are more common in children younger than 5 years and in adults older than 65 years than in other age groups. Although advances in diagnostic imaging have improved the accuracy of diagnosis in individual cases, the global rate of misdiagnosis of appendicitis remains approximately 15%, with a marked difference between females and males (22% versus 9.3%). Misdiagnosis is most common in women of reproductive age, children, and the elderly.
4. Pathophysiology
The principal cause of acute appendicitis is obstruction of the appendiceal lumen by fecaliths or lymphoid follicular hyperplasia. Fecaliths and fecal material are found in 40% of uncomplicated acute appendicitis cases, in 65% of gangrenous non-perforated appendicitis cases, and in nearly 90% of perforated gangrenous appendicitis cases. Other causes of luminal obstruction include fruit seeds, foreign bodies, parasites such as Ascaris lumbricoides, and appendiceal tumors.
Congestive (exudative) stage
Because the appendix is part of the gastrointestinal tract, its mucosa continues to secrete digestive fluids into the lumen. As the appendix is a blind-ended structure, obstruction at its proximal end causes it to rapidly fill with secretions and distend. The increased intraluminal pressure stimulates visceral afferent nerve endings, resulting in vague, dull pain around the umbilicus or in the lower epigastrium. As intraluminal pressure rises further, venous and capillary circulation becomes impaired while arterial inflow continues, leading to congestion and edema of the appendix. On longitudinal section, the mucosa appears thickened, edematous, and erythematous.
Suppurative stage
Bacterial proliferation within the lumen results in suppuration. Patients often experience nausea and vomiting as the visceral pain intensifies. The inflammatory process rapidly spreads to the serosa of the appendix and evolves into parietal peritonitis. Inflammatory exudate, pus, and fibrinous deposits may develop around the appendix. At this stage, the patient typically develops localized pain in the right iliac fossa.
Gangrenous stage
Compromise of the serosal blood supply results in progressive damage to the appendiceal wall, allowing bacteria to invade the tissue. Sluggish blood flow promotes thrombosis, and areas with the poorest perfusion are most prone to infarction. At this stage, the appendix is generally no longer salvageable. As suppuration increases, bacterial invasion and infarction lead to necrosis of the appendiceal wall and eventual perforation, most commonly at the antimesenteric border just proximal to the point of obstruction.
If a perforated appendix is not contained by adjacent bowel loops and the omentum, infection spreads throughout the abdominal cavity and progresses to generalized peritonitis. Peritonitis due to perforated appendicitis usually occurs after approximately 24 hours from disease onset. If the perforation becomes localized after 3–5 days, an appendiceal abscess may form, consisting of a pus-filled cavity walled off by bowel loops and omentum and clearly demarcated from surrounding tissues. Such an abscess may rupture into the peritoneal cavity, causing peritonitis, or may fistulize through the abdominal wall.
If non-perforated appendicitis becomes walled off by surrounding viscera after 3–5 days with absent or minimal pus formation, it is referred to as an appendiceal phlegmon. In this situation, systemic infection is mild and abdominal pain is less severe. Appendicitis may then regress. In some cases, however, the appendiceal phlegmon may become reinflamed and progress to an abscess, referred to as a phlegmonous appendiceal abscess.
5. Bacteria in Appendicitis
The bacterial flora normally present in the appendiceal lumen is similar to that of the colon. Appendicitis is not caused by a single bacterium but rather by a polymicrobial infection. The bacterial composition of an inflamed appendix differs from that of a normal appendix. Anaerobic bacteria account for approximately 60% of the flora in appendicitis, compared with only 25% in the normal appendix.
Bacteria not typically present in the normal appendix include Escherichia coli, Bacteroides spp., and Fusobacterium nucleatum/necrophorum, which are identified in 62% of appendicitis cases. Gangrenous or perforated appendicitis is commonly associated with invasion by Bacteroides species.
6. Clinical Manifestations
Typical appendicitis usually begins with dull pain in the periumbilical region or epigastrium, which later localizes to the right iliac fossa. The interval between the onset of periumbilical or epigastric pain and localization to the right lower quadrant ranges from 1 to 12 hours, most commonly 4–6 hours. Gastrointestinal symptoms such as nausea, vomiting, and anorexia may also occur.
The interval from disease onset to the appearance of clear symptoms of acute appendicitis is usually less than 24 hours. In patients presenting later than 24 hours after onset, pain may become generalized and abdominal distension may develop due to peritonitis.
Patients with typical appendicitis often appear toxic, dehydrated, tachycardic, and febrile. The severity of fever depends on whether appendicitis is uncomplicated or complicated. In uncomplicated appendicitis, fever is usually mild, generally ≤ 38.5°C. In complicated appendicitis, fever is typically higher. However, the absence of fever does not exclude the diagnosis of appendicitis.
Patients with acute appendicitis usually move cautiously and tend to lie still because of peritoneal irritation. Movement or walking may aggravate pain in the right iliac fossa. Asking the patient to cough often increases the pain in this region.
Generalized guarding or abdominal rigidity due to involuntary contraction of the abdominal wall musculature is a sign of perforated appendicitis. In cases where appendicitis has progressed to an appendiceal phlegmon or abscess, physical examination may reveal a poorly mobile mass in the right iliac fossa.

Figure 1. Clinical manifestations of appendicitis
7. Laboratory and Imaging Findings
Inflammatory markers
Complete blood count shows leukocytosis in about 90% of patients with appendicitis. In uncomplicated acute appendicitis, the white blood cell count is usually mildly elevated to >10,000 cells/mm³, predominantly with neutrophilia >70%.
An elevated C-reactive protein (CRP) level suggests appendicitis, particularly complicated appendicitis. CRP typically rises about 12 hours after the onset of inflammation.
Diagnostic imaging
Plain radiography
An upright abdominal radiograph is often obtained in emergency settings to evaluate other causes of acute abdominal pain, such as perforated hollow viscus or bowel obstruction, but it is not useful for diagnosing appendicitis.
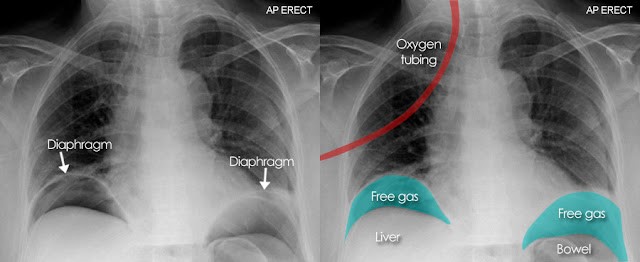
Figure 2. Perforated hollow viscus on upright chest radiograph: subdiaphragmatic free air crescent
Abdominal ultrasonography
Abdominal ultrasonography is the first-line imaging modality in patients with acute abdominal pain suspected of appendicitis because it is inexpensive, rapid, easy to perform, and free of ionizing radiation; therefore, it is especially useful in children and pregnant women. The technique used is graded-compression ultrasonography to displace adjacent bowel loops.
Ultrasonographic findings of appendicitis include a blind-ended tubular structure arising from the cecum, with a diameter >6 mm, wall thickness >3 mm, absent peristalsis, non-compressibility, a target sign on transverse view, and a finger-like appearance on longitudinal view.
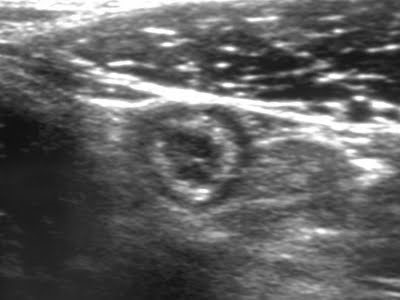
Figure 3. Ultrasonographic appearance of appendicitis
MRI
Magnetic resonance imaging (MRI) has a diagnostic accuracy of 98% to 100%. It is an alternative imaging modality for patients who should avoid ionizing radiation, such as pregnant women. MRI findings of appendicitis are similar to those seen on CT.
Abdominal CT
Abdominal CT is a highly accurate imaging modality and provides superior diagnostic accuracy compared with abdominal ultrasonography. CT findings of appendicitis include an appendiceal diameter ≥6 mm, wall thickening, surrounding inflammatory fat stranding, fluid or gas suggesting perforation, and sometimes the presence of a fecalith.
8. Differential Diagnosis
The differential diagnosis of acute appendicitis essentially includes the differential diagnosis of acute abdominal pain. Many other conditions may produce symptoms similar to those of appendicitis. Among patients who are misdiagnosed preoperatively as having appendicitis, 75% are found to have, in descending order of frequency, acute mesenteric adenitis, no detectable pathology, acute pelvic inflammatory disease, ovarian cyst torsion or rupture of a Graafian follicle, and acute gastroenteritis. The range of differential diagnoses can be narrowed based on the patient’s sex and age.
In children, the most common differential diagnoses include mesenteric adenitis following respiratory infection, acute gastroenteritis, Meckel’s diverticulitis, intussusception, and testicular torsion in boys.
In women of reproductive age, gynecologic and obstetric conditions may mimic appendicitis. These include ruptured ovarian cyst, mid-cycle pain due to ovulation (mittelschmerz), ruptured endometrioma, ovarian torsion, ectopic pregnancy, and pelvic inflammatory disease.
In the elderly, acute diverticulitis and necrotic malignant tumors of the cecum or sigmoid colon should be considered. In adults of other age groups, cecal inflammation should also be considered, as it is almost impossible to distinguish from appendicitis preoperatively.
In addition, urinary tract infection, renal calculi, and renal colic should be considered, as they may occur across multiple age groups and in both sexes.
9. Treatment
Treatment of uncomplicated acute appendicitis
The mainstay of treatment for uncomplicated acute appendicitis is appendectomy. Once the diagnosis is confirmed, intravenous access should be established and broad-spectrum antibiotics should be administered. Surgery should not be unduly delayed. Postoperative antibiotics are generally unnecessary, and most patients can be safely discharged on the first postoperative day.
Open appendectomy
The patient is placed in the supine position with slight Trendelenburg tilt and slight left lateral tilt. The surgeon may enter the abdomen through a McBurney oblique incision, a Rockey-Davis transverse incision, or a midline incision. The cecum is grasped by the taeniae coli and delivered into the wound. The base of the appendix is identified at the convergence of the three taeniae coli. Adhesions around the appendix are released. The mesoappendix is divided, the appendix is transected close to its base, and the appendiceal stump is ligated.
Laparoscopic appendectomy
The patient is also placed supine with slight Trendelenburg tilt and slight left lateral tilt. The surgeon stands on the patient’s left side. A urinary catheter is inserted. The abdomen is entered with a 10-mm trocar at the umbilicus for the laparoscope. Two additional trocars are usually inserted, one in the left iliac fossa and one suprapubically. Alternatively, a trocar may be placed in the right iliac fossa instead of the left, which is advantageous if drainage is needed in the right iliac fossa. The appendix and its base are identified by locating the convergence of the three taeniae coli. The mesoappendix is grasped and divided close to the base using monopolar cautery, bipolar cautery, or an ultrasonic scalpel. The base of the appendix is ligated with a Roeder loop and transected, and the appendix is removed. Inflammatory fluid in the right iliac fossa and Douglas pouch is irrigated and aspirated, after which the abdomen is closed.
Treatment of perforated appendicitis
Patients with signs of peritonitis require immediate surgery. Preoperative resuscitation is similar to that for uncomplicated appendicitis. After appendectomy, the abdominal cavity should be thoroughly irrigated and all fecaliths removed. Broad-spectrum antibiotics are continued postoperatively for 4–7 days.
10. Special Situations
Appendicitis in pregnancy
Appendicitis is the most common non-obstetric surgical emergency during pregnancy. It may occur at any stage of gestation but is less common in the third trimester. About 50% of cases occur during the second trimester. The rate of negative appendectomy in pregnant women is approximately 25% to 50%, much higher than in non-pregnant women.
Only about 50% to 60% of pregnant patients present with typical symptoms of acute appendicitis. Gastrointestinal symptoms are often nonspecific and may be confused with common symptoms of pregnancy. Anatomical changes caused by the enlarging uterus also affect abdominal examination. In the second trimester, pregnant women often experience lower abdominal pain due to stretching of the uterine ligaments, which can easily be mistaken for appendicitis.
The risk of preterm birth is approximately 11% and the risk of miscarriage approximately 6% in pregnant women with complicated appendicitis, compared with 6% and 2%, respectively, in uncomplicated appendicitis. Even in cases of negative appendectomy, the corresponding rates are still about 10% and 4%.
Appendicitis in children
The diagnosis of acute appendicitis in children is much more difficult than in adults because children are often unable to provide an accurate medical history, and common pediatric gastrointestinal illnesses are frequent, leading to delayed diagnosis. Perforation progresses rapidly because children do not yet have a well-developed greater omentum, resulting in a higher rate of complications. In children younger than 5 years, the negative appendectomy rate is approximately 25% and the perforation rate about 45%, whereas in children aged 5–12 years the corresponding figures are <10% and 20%, respectively.
Appendicitis in the elderly
Although appendicitis is less common in the elderly, its diagnosis is often more difficult because clinical manifestations are frequently atypical, there are many alternative diagnoses, and communication may be challenging. Consequently, the perforation rate in elderly patients is high, ranging from 50% to 70%, and is particularly common in those older than 80 years. Elderly patients often complain of lower abdominal pain without the typical localization to the right iliac fossa seen in younger individuals. The classic pattern of periumbilical pain migrating to the right lower quadrant is less common in this age group. Perforated appendicitis should be suspected in elderly patients with fever >38°C, neutrophil percentage >76%, especially in male patients, anorexia, and abdominal pain lasting several days.
REFERENCES
- Le, Van Them. “Clinical characteristics of patients with acute appendicitis treated at Saint Paul General Hospital in the first quarter of 2021.” Vietnam Medical Journal 512.2 (2022).
- Bryon R. (2016). “The Appendix.” In Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice, 20th edition. Elsevier, Canada, pp. 1296–1311.
- Quadri, Rehan, et al. “Comprehensive review of typical and atypical pathology of the appendix on CT: cases with clinical implications.” Clinical Imaging 53 (2019): 65–77.
- Pai, Sanjay A., and Rifat Mannan. “Nonneoplastic pathology of the appendix: A review article, based on the recent literature.” American Journal of Clinical Pathology 161.5 (2024): 418–429.
Herrod, Philip J.J., Alex T. Kwok, and Dileep N. Lobo. “Three centuries of appendicectomy.” World Journal of Surgery 47.4 (2023): 928–936. - Lotfollahzadeh, Saran, Richard A. Lopez, and Jeffrey G. Deppen. “Appendicitis.” StatPearls [Internet] (2024).
- Spanos, Constantine P., and Constantine P. Spanos. “Appendicitis.” In Acute Surgical Topics: An Infographic Guide (2021): 17–28.
MSc. Kim Ngoc Son
MSc. Tran Khanh