Health communication
CONTENTS
Food allergy
1. Definition
Food allergy refers to adverse reactions resulting from an abnormal immune response to specific protein components present in food. These reactions may be mediated by IgE, non-IgE mechanisms, or a combination of both. Food allergy affects approximately 5–8% of children and 2–4% of adults. The most common food allergens in children are cow’s milk, eggs, and peanuts, whereas in adults, seafood, fish, peanuts, and tree nuts are the most frequent triggers.
2. Pathophysiology
Food allergy is predominantly an immediate hypersensitivity reaction (type I), with clinical symptoms developing rapidly, from a few minutes to several hours after exposure to the offending food.
Upon re-exposure, the allergen binds to specific IgE antibodies already attached to FcεRI receptors on mast cells. The cross-linking of two IgE antibodies by one allergen facilitates the release of inflammatory mediators such as histamine and serotonin, leading to clinical manifestations including erythema, urticaria, pruritic papules, and angioedema.
3. Clinical Manifestations
Clinical manifestations are diverse and complex, depending on factors such as age, the type of food involved, and the underlying immunologic mechanism.
Urticaria
This is the most common manifestation, typically occurring from a few minutes to one hour after food ingestion. Patients often experience flushing, pruritus, and edematous wheals on the skin. Scratching tends to exacerbate the lesions and promotes their rapid spread.
Angioedema
Angioedema is common and presents as marked swelling of the lips, neck, eyelids, genitalia, or extremities. The lips are among the most frequently affected sites.
Allergic bronchial asthma
An episode of acute dyspnea may develop rapidly after food ingestion.
Allergic rhinitis and allergic conjunctivitis
Nasal symptoms such as nasal obstruction, nasal pruritus, and rhinorrhea, together with ocular symptoms including conjunctival hyperemia, itching, and tearing, usually develop within minutes to one hour after ingestion and are often accompanied by systemic manifestations such as urticaria and angioedema.
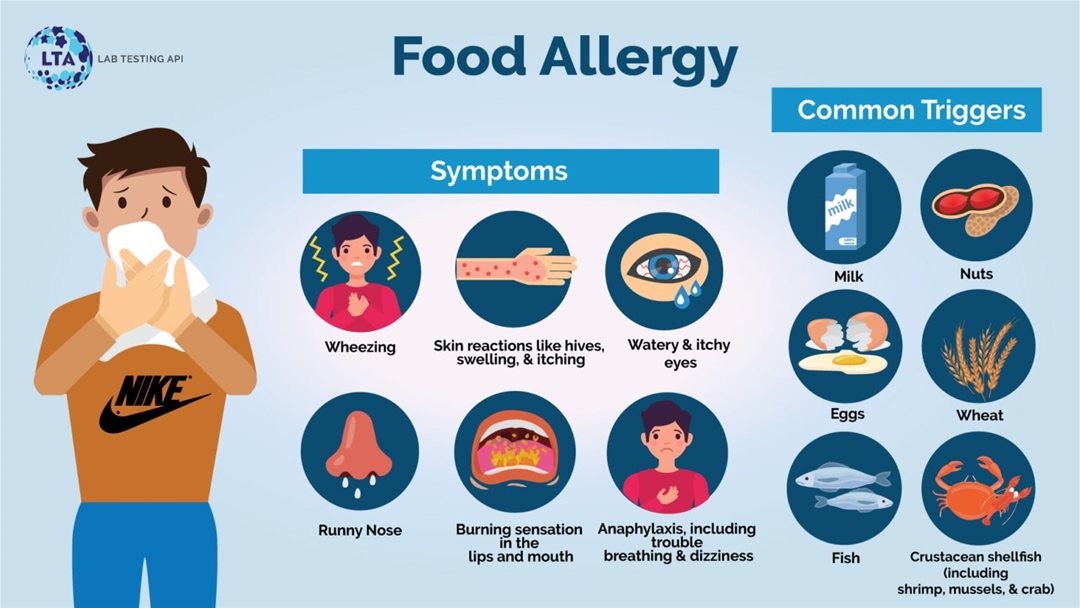
Figure 1. Clinical manifestations of food allergy
Oral allergy syndrome
Clinical manifestations include itching in the oral cavity, swelling of the lips, swelling of the tongue, and sore throat.
Anaphylactic shock
This is the most severe clinical presentation and may manifest in various ways. It may occur together with urticaria or as isolated anaphylaxis. After exposure to the offending food, patients may develop malaise, anxiety, restlessness, generalized pruritus, crampy abdominal pain, a rapid thready pulse, progressive hypotension, severe dyspnea, followed by coma, convulsions, urinary and fecal incontinence, and death.
Generalized erythroderma
Initially, patients may experience generalized pruritus, fever, gastrointestinal disturbances, and rash. This is followed by diffuse erythema with white scales of varying sizes and fissuring of the hands and feet.
4. Foods That May Cause Allergy
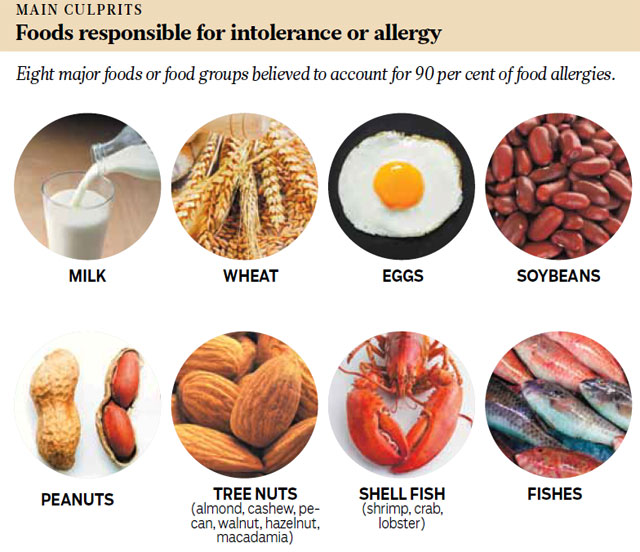
Figure 2. Foods that may cause allergy
Cow’s milk protein allergy
Cow’s milk protein allergy appears very early in infancy and is caused by milk proteins, mainly casein and whey. Clinical manifestations include rhinorrhea, wheezing, urticaria, angioedema, lacrimation, and vomiting, with symptoms usually developing abruptly within minutes to one hour.
Egg allergy
Egg allergy accounts for approximately 30% of food allergy cases in children and about 7% of food allergy cases in adults. Chicken egg allergy is the most common form, and several proteins in egg white are capable of inducing allergic reactions.
Fish and shellfish allergy
Marine fish such as tuna, cod, sardine, and salmon may trigger allergic reactions. Shellfish, including shrimp and crab, are also common allergens. Proteins implicated in this group include tropomyosin, arginine kinase, sarcoplasmic calcium-binding protein, troponin C, triosephosphate isomerase, and actin.
Wheat allergy
Wheat allergy is more common in children than in adults. Clinical symptoms usually occur immediately after wheat ingestion but may also develop 5–6 hours later.
Allergy to peanuts, soybeans, and tree nuts
Peanut allergy may cause severe and potentially life-threatening reactions. Soybean allergy commonly causes allergic reactions in children. Tree nuts such as walnuts and almonds are also common food allergens.
5. Diagnosis
Clinical history
A detailed medical and dietary history is considered the first effective tool for identifying the likely food allergen. Examples of key questions include:
- When did the symptoms occur?
- What type of food was consumed?
- Was the food cooked or raw?
- Did others who shared the same meal develop similar symptoms, or was only one person affected?
- Has the patient had a similar reaction to the same food previously? If so, did the severity depend on the amount consumed?
After collecting this information, the clinician can identify foods suspected of causing allergy. The following diagnostic methods may then be used to confirm the offending allergen.
Oral food challenge
This test is performed in a hospital setting because medical supervision is required. It may be conducted as an open, single-blind, or double-blind food challenge.
Elimination diet
The suspected allergenic foods are first completely eliminated from the diet and then reintroduced over a period of time for observation.
- If allergic symptoms persist during the elimination diet, the excluded foods are unlikely to be the causative agents.
- If symptoms resolve after elimination of a certain food and recur after reintroduction, that food is considered the offending allergen.
Skin prick test with food allergens
The skin prick test is a technique in which a needle is used to introduce a drop of food allergen extract through the epidermis to assess the degree of allergic reactivity. Results are read after 15–20 minutes. A reaction is considered positive based on the maximal wheal diameter (≥3 mm), surrounding erythema, and pruritus, compared with the negative control (distilled water) and positive control (histamine) (Figure 4).
Blood test for serum IgE antibodies
Measurement of serum IgE antibody levels may also aid in the diagnosis of food allergy.
6. Treatment
A diet free of the causative food allergen is the most effective treatment strategy.
Suppression of inflammatory mediators
- H1-antihistamines: This is the most important drug class for the treatment of symptoms caused by allergic mediator release. Examples include diphenhydramine, hydroxyzine, loratadine, fexofenadine, and desloratadine.
- Oral or injectable corticosteroids: These are used in severe allergic reactions. For example, methylprednisolone may be administered at 0.5–1 mg/kg/day, with a maximum dose of 80 mg, and tapered once symptoms improve.
- Symptomatic treatment: Includes antipyretics, bronchodilators, and agents to reduce intestinal smooth muscle spasm in the management of shock-related symptoms.
- Epinephrine: This is the most important drug in the treatment of food allergy–induced anaphylactic shock.
- Children weighing 10–25 kg: epinephrine 0.15 mg intramuscularly
- Children weighing >25 kg: epinephrine 0.3 mg intramuscularly
- Adults: epinephrine (1:1000) 0.01 mg/kg per dose, up to a maximum of 0.5 mg per dose
- Epinephrine may be repeated every 5–15 minutes if necessary.
REFERENCES
- Kotra, A., Chaudhary, N., & Jabalia, N. Role of Bioinformatics in Food Allergens: An Overview, 2015.
- Simons, F.E.R. (2003). Antihistamines. Allergy: Principles and Practice, 6th edition, vol. 1. Philadelphia: Mosby, 834–869.
- James, J.M., Burks, W., & Eigenmann, P. (2012). Food Allergy. Saunders, Toronto.
- Sampson, H.A., & Burks, A.W. (2008). Adverse Reactions to Foods. Middleton's Allergy: Principles & Practice, 7th edition, Mosby, 1139–1169.
- Sharma, S. (2021, March 26). Food allergy: Causes, symptoms, diagnosis, and treatment. Lab Testing API.
- Allergy testing. (2014, March 7). Kallergy.
MSc. Kim Ngoc Son
MSc. Nguyen Duong Ngoc Thoi